There are four main ligaments that stabilize the knee. They contain or restrain motion between the thigh bone (femur) and leg bone (tibia). They perform the important function of maintaining knee stability for walking , pivoting, turning and almost any athletic activity. The four main ligaments are: the anterior cruciate ligament, the posterior cruciate ligament, the medial collateral ligament, and the lateral collateral ligament. There are also a number of smaller yet important ligaments that contribute to knee stability.
Most knee ligament injuries involve a single ligament injury, such as an isolated anterior cruciate ligament, medial collateral ligament or posterior cruciate ligament tear. When there is major trauma such as a direct blow to the knee, or a fall from a height, or motor vehicle trauma several knee ligaments can be torn at the same time. This is the “multiple knee ligament injury.” This requires specialized attention and treatment. Many patients with this injury have had other injuries to the chest, abdomen, etc. which take precedence in treatment over the knee injury. Many of these injuries to several ligaments result in a knee dislocation.
This is an emergency and often requires reduction or the physician or surgeon to put the knee back into place. A percentage of these patients will have a nerve injury at the level of the knee or even have a severe artery injury requiring treatment. Again, these injuries require immediate attention and patients will have various immediate treatment such as an arterial graft and external fixator applied to hold the knee in place while these other injuries heal.
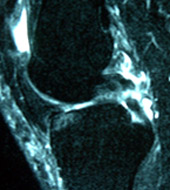
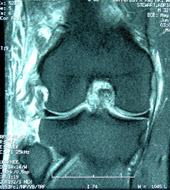
At the UConn Musculoskeletal Institute, patients will be referred for attention to the multiple knee ligament injuries. Patients will complain of severe instability and disability that is adversely affecting every day life, work and sports participation. When the surgeon examines these patients, the knee will be very unstable and demonstrates exam findings that implicate more than one ligament being damaged. We have seen a number of combined knee ligament injury patterns such as: 1) anterior cruciate ligament and posterior cruciate ligament tear with tears of the posterolateral corner and 2) anterior cruciate ligament and posterior cruciate ligament tear with tear of the medial collateral ligament. In addition to the physical exam and X-rays, an MRI (magnetic resonance image) will display and confirm the presence of injury to multiple knee ligaments (see Figures 1A and 1B).
The treatment of these very severe knee ligament injuries almost universally requires surgery. Rarely, in the most sedentary and low demand patients, bracing and rehabilitation will diminish the instability complaints. For most other patients, a very involved surgical reconstruction is required. Because surgical correction involves the reconstruction of several ligaments, the surgeon often will utilize grafts or tendon tissue from cadavers or human donors. Sometimes the surgeon will select tendon grafts from the patient and from a donor.
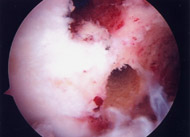
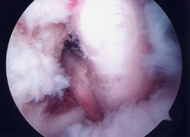
The surgical reconstruction takes a dedicated team and is a very technically demanding procedure. This type of surgery is best performed by surgeons with experience with these procedures and one that performs a number of these procedures on an annual basis. The surgeon will use the arthroscope, a small instrument that is inserted into the knee that is connected to as camera and monitor. Often several of the ligaments will require reconstruction to include the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL) and collateral ligaments (see Figures 2A, 2B).
The surgeon will use the arthroscope to create tunnels in the thigh and tibia bone with a small drill that will permit the grafts to be placed into the knee and re-create the torn ligaments. The tunnels are made in the exact anatomic positions where the normal ligaments were attached. Once the grafts are placed they are secured to the bone with screws, washers, and other fixation devices. These devices are important to hold the ligament in place until the patients bone heals to the ligament. This process takes nearly three months to get really strong. That is why most patients will have to use crutches for 6 to 8 weeks and why the rehabilitation is typically much slower than for a single ligament injury such as an isolated anterior cruciate ligament tear.
Because the surgery is very extensive the risk of complication is higher. The most common complication is recurrent instability. At the opposite spectrum patients may develop stiffness or loss of motion. Rarely, the patient will require a manipulation or a repeat arthroscopic procedure to remove scar tissue. Because the surgery is performed around major nerves and blood vessels, injury to these structures can occur which may demand additional surgical treatment. Fortunately, these more severe complications are rare but emphasizes the need surgery to be performed by experienced surgeons.