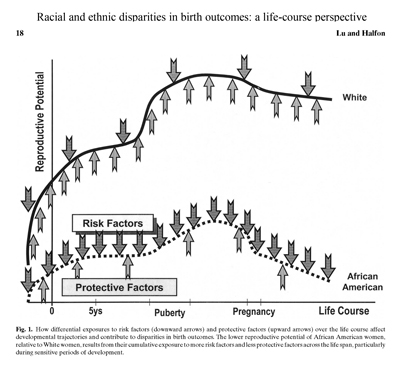
Health Disparities (HD) are notoriously hard to identify reliably; moreover finding what causes them, and hence how to reduce and eliminate them, is especially difficult, but models exist (see the Framework for Health equity below, the birth outcomes illustration, and other conceptual and practical models).
The main reason is that simple group comparisons of a health outcome is not enough to conclude that HDs exist, and to what extent they do. Such group comparisons need to ‘take into account’ outside causal factors (like neighborhood, or socio-economic conditions) that ‘partially explain’ the raw difference we notice at first. We can provide advice on such matters, e.g.:
- How and why and what to ‘control for’ when deciding the extent of HDs is what we can provide assistance with, to researchers but also community stakeholders interested in extracting and translating evidence, so that it can become actionable.
- How can one distinguish between: inequities/differences/disparities/discrimination. There are ways to test for discrimination, one involving assessing residual direct effects after explaining other mechanisms that may operate, or specific mediators like implicit prejudice.
- How can make causal claims in the HD world:
3.1. Can race/ethnicity ‘cause’ health outcomes? Can gender cause them? It is debatable, but there are ways to handle this better/worse.
3.2. What not to ‘control for’ when comparing groups: an intermediate outcome is problematic for example, others even more problematic.

3.3. Various matching methods exist that allow for true comparability; such matching may induce at times relationships between variables that are not manifest in the entire population.
3.4. Instead of having race/ethnicity ‘cause’ health, one can compare populations in simple and complex ways of causal relationships.
- How to apply a person/patient-centered view to HDs: what can statistics tell us about Darnell‘s vs. Jake’s vs. Jose’s health outcomes, and how can this provide feedback to their health care providers.
3.4. A practical solution is to find completely identical Darnell and Jake and compare their patient experiences and outcomes.
- Measuring race and ethnicity are the pillars of HD answers, yet these are difficult to measure reliably, better solutions exist of course.
- We can specifically help with gathering, processing and analyzing health data to develop health disparities dashboards/reports for health care providers of other stakeholders interested in this.
We list below some modeling resources (papers, software code for analyses, outputs) that refer to some of our prior work.